Chapter XII
[See also History of the Medical Department of the U.S. Navy in World War II --HyperWar]
Bureau of Medicine and SurgeryTHE STORY of the warship doctor in the United States begins concurrently with the history of the Navy. At the very outset of the Revolution in 1775, when the Continental Congress resolved to outfit a naval force, provision was made for the inclusion of surgeons in ships' complements. Ships of 20 or more guns were to carry a surgeon, and smaller vessels a surgeon's mate having warrant officer status. A surgeon's pay in the Continental Navy was originally set at $25 a month, later raised to $30; in 1777, Congress provided that no one was to be appointed surgeon or surgeon's mate without a certificate of examination attesting to his professional qualifications. Until 1942, candidates for a commission in the Medical Corps of the United States Navy were required by law to be examined before a board and to pass comprehensive examinations. After that year, a diploma of graduation from a medical school that had the approval of the American Medical Association and an examination of the candidate's record were substituted for the written examinations. Historical Background
In the earliest days, the surgeons of the individual ships acted independently of each other and there was no provision for coordinating and supervising their activities. A step toward organizing military medicine was taken by Congress in an Act of March 2, 1799, providing for a physician-general "charged with the superintendence and direction of all military hospitals, and generally of all medical and chirurgical practice or service concerning the Army or Navy of the United States"; for an apothecary-general "who will be charged with the safekeeping and delivery of all medicines, instruments, dressings and other articles"; and for a purveyor "who shall be charged with providing medicines, stores, and whatsoever else may be necessary in relation to the said practice or service."1
The title of surgeon's mate was changed in 1828 to Assistant Surgeon, and the same enactment called for the appointment of an experienced
surgeon in the naval service to every fleet or squadron, to be designated "Surgeon of the Fleet" and "who shall be surgeon of the flagship and who, in addition to his duties as such, shall examine and approve all requisitions for medical and hospital stores for the fleet and inspect their quality; and who shall, in difficult cases, consult with the surgeons of the several ships, and make records of the character and treatment of diseases, to be transmitted to the Navy Department.2It is clear that a Medical Department had by 1828 become a well recognized part of the Navy, afloat and ashore. Apparently, however, it received little administrative attention from Washington. This was changed by an Act of Congress approved August 31, 1842, abolishing the Navy Commissioners and distributing their duties among five bureaus, one of which was named the Bureau of Medicine and Surgery.
The Bureau of Medicine and Surgery is unique in that it is the only one of the five original bureaus whose name has not been changed, whose responsibility and duties are fundamentally the same as they were when the Bureau system was adopted and which escaped most of the strife over cognizance that characterized the Bureau system from the beginning, especially during its early days. All of this resulted from the highly specialized nature of the medical profession.
While there were after 1842 conflicts over bureau cognizance generally, there was from the beginning never any argument about the scope of the Bureau of Medicine and Surgery's responsibilities. That Bureau was clearly intended, as later elaborated in Navy Regulations, to have the responsibility for safeguarding the health of the Navy, for the care of sick and injured naval personnel, for keeping their health and medical records, and for setting the professional standards for its physicians, dentists, nurses, and other Medical Department specialists. The medical care of the dependents of naval personnel was also gradually added to these responsibilities. The scope fo Medical Department and BuMeed activities expanded greatly over the years to keep the Navy's medical and dental practices in step with the advances in Medical and dental science in civilian life and to make iut possible for the Navy to make its own contribution to medical and dental progress.3
The term "medical department" was employed in the Navy to describe an important naval activity long before the Bureau of Medicine and Surgery was created. "Medical Department of the Navy" is still used as a collective term to encompass the overall responsibilities of the Bureau of Medicine and Surgery throughout the Naval Establishment.In ships, the term "medical department" is used to designate specifically an organizational segment of the ship. Actually, for the smallest of naval craft it may consist of only a first aid kit, or for such vessels as submarines, destroyers, etc. there may be a hospital corpsman with his more complete equipment. On the largest ships, the medical department is under the direction of a medical officer, and with a dental department under the direction of a dental officer, each with their professional assistants and full equipment. A still more complete medical and health service is provided in hospital ships with their complement including women nurses.
On shore, the range in the size of medical departments is even greater than it is afloat. None of the Navy's shore establishments is without its medical department whether merely an officially furnished first aid kit for the smallest activities or a well equipped dispensary for its large establishments. All of these activities, both afloat and ashore, are under the technical control of the Bureau of Medicine and Surgery. The Bureau has management control, as well, of all naval hospitals and by the end of World War II operated 40 additional activities such as hospital corps schools, research units, and preventive medicine units. As in the case of all other activities of the Navy Department, military jurisdiction over the medical department and its naval personnel rests with district commandants and ship commanders. The Bureau of Naval Personnel handles most of the minutia connected with the recruitment, service records, assignment to minutia connected with the recruitment, service records, assignment to duty, etc., of medical departments personnel, as it does for all other naval personnel; but BuMeed is responsible for everything having to do with the professional qualifications, professional assignments, standards of competence, and promotion of medical department personnel.
Going back again for a moment to BuMeed early history, Doctor William P.C. Barton, second on the list of naval surgeons, was selected by President Tyler in 1842 as the first Chief of the Bureau of Medicine and Surgery. For a number of hears the personnel of the Bureau consisted of Dr. Barton and two clerks. With this small force he inaugurated many procedures to improve and standardize the practices of medical departments both afloat and ashore and to raise the professional standards of medical officers. He started the publication of a naval medical journal and made provision for medical libraries at the principal naval medical activities.4 In 1871, Congress authorized the title of Surgeon General with
the relative rank of Commodore for the Chief of the Bureau of Medicine and Surgery.During World War II, the naval personnel of the Medical Department of the Navy consisted of the following corps, and were represented in the organization of the Bureau of Medicine and Surgery. All played a part in the administration of the Navy Department during the war.
Medical Corps. The Medical Corps consists of the medical officers in the naval service. Navy Regulations of 1865 designated surgeons as staff officers and set the relative rank between them and line officers, Surgeon of the Fleet ranking with Captain, down to Assistant Surgeons who ranked with Masters. The heated controversy over rank between the Staff Corps, including the Medical Corps, and the line of the Navy reached its peak in the years immediately following the Civil War. In 1899, medical officers gained a point in this controversy when Congress abolished relative rank and gave staff officers actual rank.5 Naval Personnel of the Medical Department
The number of doctors on the active list of the Navy is controlled by Congress. An Act in 1916 established the authorized strength of the Medical Corps at 0.65 of one percent of the total number of the officers and enlisted men of the Navy and Marine Corps, including midshipmen.6 This was the statutory limitation in effect during World War II. The actual number was limited by the amount of money appropriated for the actual number was limited by the amount of money appropriated for the pay of the Medical Corps. In peacetime, the actual strength has seldom equalled the statutory limit.
To provide a pool of doctors available for call to fill the needs of an expanding Navy in time of national emergency, Congress established a Medical Reserve Corps in 1912 as an integral part of the Medical Department.7 Reserve medical officers were called to duty in large numbers during World War I, and likewise made possible the vast expansion of the Medical Department in World War II. In July of 1940, there were 932 Medical Corps officers on active duty.8 By June 30, 1945, this number had grown to 13,764, of which 11,666, or almost 85%, belonged to the Medical Reserve Corps.9
Dental Corps. Before 1912 there were no dental officers in the Navy.
The Naval Appropriation Act, passed on 22 August of that year, made provision for the appointment of not more than 30 assistant dental surgeons. They were to be a part of the Medical Department of the Navy, to receive the same pay and allowances, and to take rank in the same manner as Medical Corps officers. When deemed necessary the Secretary of the Navy was empowered to appoint additional dental officers for temporary service, not to exceed the proportion of one dentist to every one thousand of the authorized enlisted strength of the Navy and Marine Corps.10ALthough a Naval Dental Corps was not established by that name by the 1912 Act, the language of the Act implied that such was the intent of Congress. A Naval Dental Reserve Corps was authorized in 1913, to be operated and administered in the same manner as the Medical Reserve Corps The authorized strength of active duty dental officers was set, in 1935, as one for each 500 of the actual number of officers and enlisted men in the Navy and Marine Corps In December 1941, there were 759 dental officers on active duty. This number grew to 7,026 by September 30, 1945, of which 91.5% were reservists.
Hospital Corps. Toward the end of the 19th century, the Surgeon General had, on a number of occasions, recommended a Hospital Corps to provide male nurses to attend the sick on board ship and to perform other special duties in the Medical Department. The Spanish-American War brought the need for such a Corps to a head and led Congress to pass an Act on June 17, 1898, establishing the Hospital Corps of the Navy, to consist of "tenty-five pharmacists with the rank, pay, and privileges of Warrant Officers, to be appointed by the Secretary of the Navy and removable at his discretion, and as many hospital stewards, hospital apprentices, first class, and hospital apprentices as in the judgements of the Secretary of the Navy were necessary and that it should be attached permanently to the Medical Department of the Navy."11
The authorized strength of the Hospital Corps was set in 1916 at "3.5 percent of the authorized strength of the Navy and the Marine Corps and shall be in addition thereto."12 The Hospital Corps numbered about 6,000 officers and enlisted men in 1940, and expanded to approximately 3,500 officers and 130,000 enlisted men and women by the end of World War II, a figure approximately equal to the entire strength of the U.S. Navy in 1937.13
During World War II, outstanding warrant and chief warrant officers
were given temporary promotions for the duration of the war up to and including the rank of Commander. In order to vive permanent status to qualified officers in this category, and to provide career opportunities for the numerous medical specialists and technicians who became an essential element of the Medical Department in World War II, the Medical Service Corps was established by Congress in 1947. It consists of commissioned officers in such specialties as supply, optometry, pharmacy, and other medical specialties.14 When a member of the Hospital Corps is eligible for rank above chief medical service warrant officer, he is transferred to the Medical Service Corps.Nurse Corps. Although the female Nurse Corps of the Navy was not established until 1908, the Navy during the Civil and Spanish-American Wars had made use of women nurses. Between 1902 and 1904, several bills were introduced in Congress to create a Nurse Corps, but failed of passage. The 1908 law, which established the female Nurse Corps, provided for the appointment of graduate nurses after passing professional and physical examinations. The head of the Corps, appointed by the Secretary of the Navy, is designated Superintendent of Nurses. Nurses are assigned to duty at naval hospitals, naval dispensaries, on board hospital ships, or to such other duties as approved by the Secretary of the Navy.
World War II saw the Nurse Corps grow from about 800 to over 11,000, of which 83.6% were reserve nurses. An Act of December 22, 1942 granted members of the Nurse Corps relative rank, but not commissioned status, for the duration of th e war and six months thereafter.15 Relative rank was changed to actual rank in February 1944.16
As the Navy does not give basic training to its medical doctors, dentists, and women nurses, candidates for appointment to these branches of the uniformed service must have received their professional education and basic training before applying for appointment. In World War I, the Navy's needs for medical and dental personnel were met by the regular establishment, the existing reserve, and by enrolling additional doctors and dentists as reserves. When hostilities ceased there was actually a large pool of reserve medical officers on whom no call had been made.17 Procurement of Medical Department Personnel
Rear Admiral Percival S. Rossiter (MC)
Chief of Bureau of Medicine and Surgery, 1933-1938.The Bureau continued its efforts during the inter-war period to keep the medical profession in civilian life interested in the medical reserve of the Navy.18
In 1940, the Bureau invited the reservists to report for active duty, and most of them responded. They were invaluable in providing a trained nucleus for the later expansion of BuMeed activities.
Planning. World War I had underlined the need for advance planing to cope with a national emergency such as confronted the country when
World War II broke out in Europe. The Surgeon General called a full dress planning conference immediately, which dealt with necessary expansion in the fields of personnel, logistics, and facilities. An increase in appropriations was an immediate need. The appropriation for BuMeed had for some years averaged about $13,000,000 annually, but was about double that amount for fiscal 1939. It was increased to $50,000,000 for fiscal 1940, and rose to about $500,000,000 annually for the later years of the war.In planning for personnel, the Chief of the Bureau recalled Rear Admiral E.R. Stitt, (M.C.), USN, a former Surgeon General, to active duty, and had him visit medical and dental schools to enlist their aid in getting young doctors and dentists to join the Navy. Admiral Stitt was world renowned as an expert in tropical medicine and was very effective in his professional contacts with civilians.
The Surgeon General also selected a number of personable young medical officers to visit secondary schools to encourage enlistments in the Hospital Corps. Those so obtained were among the best recruitss that joined the Navy and later became key figures in the Corps. Their intelligence level and motivation averaged higher than that of the draftees obtained later on.
The steps taken to implement the plans for personnel procurement and expansion of facilities and supply will be covered in more detail in later pages.
Ax one of the lessons learned from the war, Admiral McIntire summarized the factors that contributed to the speed and effectiveness of early BuMeed planning. He pointed out that the planning was, in the first place, single service planning to meet the specific needs of the Navy, and that these needs were not too difficult to visualize. There were relatively few echelons through which the plans had to pass before reaching the Secretary of the Navy for final decision, and that it was not difficult for the Surgeon General to see the Secretary at any time. Considerably less clearance with the Chief of Naval Operations was necessary than later on. And most important of all, there was at that time no third echelon above all of the services, through which plans had to be cleared and which had the power to stop programs at any stage in their execution. Admiral McIntire summed up this aspect of postwar planning and administration by saying, "When you lengthen the chain of command, you weaken the whole system."19
Planners were able to concentrate on determining what personnel, medical facilities, and suppliers would be needed to support the planned Combat Operations of the Navy. The plans visualized peaks rather than
averages, the maximum number of casualties that might occur in a given operation rather than a figure representing a former average. If this had not been the practice, medical support for the operating forces would often have been found inadequate to meet the requirements.Procurement and Assignment Service. In October 1941, an Executive Order created the Procurement and Assignment Service within the Office of Defense, Health, and Welfare Service (a national war emergency organization) for the purpose of receiving requests for medical and dental personnel from various government agencies; securing and maintaining lists of available professional personnel together with details of their qualifications; and stimulating interest in volunteering for military service in this field. The Procurement and Assignment Service was headed by a policy-forming board of five eminent physicians service without compensation.20
The status of the Procurement and Assignment Service as a national coordinating agency required BuMed to alter its procurement practices which previously had been direct with prospective civilian candidates. BuMed now made the Navy's needs for physicians and dentists known to the P& Service, which in turn supplied BuMed with a list of names approximately 30 percent larger than needed. The Bureau then got in touch with the individuals on the list to ascertain their interest in naval service. BuMed submitted completed applications to the P&A office for comment and record purposes before forwarding them to BuPers for entrance action.21
In a number of instances during the war, eminent specialists, who actually preferred naval service, entered the Army because they were offered commissions with rank one or more grades higher than the top grade, Lieutenant Commander, permitted for Navy entrants.22
Requisitions for physicians and dentists by all claimants, civilian and military, exceeded the number in actual practice even after adding those about to graduate from professional schools. Therefore, with the approval of the Director fo Selective Service a formula was put into effect which allowed the Navy to commission qualified students in medical and dental schools as Ensigns, USNR, in an inactive status. Similarly qualified pre-medical and pre-dental school students were enlisted as Seamen Apprentices in the Naval Reserve, to receive later an Ensign's commission if accepted by a class "A" professional school.23
Rear Admiral Ross T. McIntire (later Vice Admiral) (MC)
Chief of Bureau of Medicine and Surgery, Dec. 1938-Dec. 1946When the Army and Navy notified the P&A Service that 42,000 additional military physicians would be required by the end of 1942, the P&A advised that this need was rapidly approaching the maximum consistent with maintaining essential civilian health services.24 In the fall of 1942 procurement of physicians by BuMed was restricted to the five states (New York, Massachusetts, Pennsylvania, California, Illinois) where the civilian shortage was the least acute.
To tap another source the Navy began accepting applicants from non-class "A" medical schools. Unlike graduates of accredited medical schools, these men had to submit to oral, written, and practical examinations.25 As a further expedient, the Secretary of the Navy approved the Surgeon General's recommendation of 18 February 1943 that female physicians be accepted in the Navy, to release male medical officers for duty afloat and overseas.26 In addition, a shortened internship and residency which was approved by the Procurement and Assignment Service, the State licensing boards, and the armed services, made young physicians more quickly available for military duty.27 Later, the age limit for acceptance of physicians was raised to 55, and the physical requirements were lowered.V-12 Program. By far, the greatest source of prospective physicians and dentists for naval service during World War II, was the V-12 college training program which went into effect on 1 July 1943. This program superseded previous pre-professional and professional training programs, and provided for enlisting qualified undergraduate and professional students as Apprentice Seamen, USNR, in an active status. So long as they remained physically and academically qualified the tuition and incidental expenses of V-12 students were paid by the Government, and they received active duty pay in addition. They were in that way removed from the jurisdiction of Selective Service. Removed, also, was the objection to the earlier program that it favored exemption from the draft of individuals financially able to continue their education. However, those students who failed to maintain required standards were transferred to general duty in the Navy. The Navy's quota of V-12 medical and dental students, arrived at by mutual agreement with the Army and the War Manpower Commission, was 25% and 20%, respectively, of the total school enrollment.28
During the operation of the V-12 program, some 4,600 medical and dental students completed their professional training in addition to another 5,000 medical and nearly 1,400 dental students who received a part of their professional education in this way. By the end of the war, approximately 23 percent of the Navy's medical officers and 20 percent of the dental officers had passed through the V-12 program.29
As of 30 June 1945, there were 13,764 Medical Corps officers on active duty in the Navy. It is of interest to note that at the beginning of the war there was one medical officer for every 142 persons in the naval service,
whereas on 30 June 1945, there were 281 service persons for each medical officer.30 Thus, in addition to the extra burdens occasioned by combat operations, each medical officer carried an average load twice that of pre-war years.Nurse Procurement. Registered nurses, in a similar manner to physicians, were entered on the rolls of the Procurement and Assignment Service on the basis of their availability for military service. The Red Cross is credited by BuMed with playing a major role in getting in touch with student and graduate nurses to recruit them for duty in the Navy Nurse Corps.
Although early in 1945 a proposal was made in Congress to enact legislation authorizing a nurses' draft this never became necessary.31 The possibility, however, may have stimulated recruiting, for by mid-April 1`945 the Navy found itself with a surplus of 500 applicants. As there was no need for them in the Navy, they were urged to join the Army.32
Inasmuch as those entering the Medical, Dental, and Nurse Corps must be graduates in their professions, further instruction after joining the Navy is given them at the postgraduate level. It is designed as orientation to ready them for the specialized demands of naval service afloat and ashore. Furthermore, many of the duties, professional, administrative, and military performed by Medical Department personnel are not ordinarily encountered in civilian practice. Personnel Training
Naval Medical School. Surgeon General James Rufus Tryon can lay claim to being the father of the modern Naval Medical School. In 1893, Tryon ordered the establishment of a Department of Instruction at the United States Naval Hospital, Brooklyn, New York, where "Assistant Surgeons shall, immediately after admission to the Navy, be ordered . . . for such duty and instruction . . . as may be necessary to familiarize them with the duties of medical officers afloat and on shore."33 A course lasting three months was given. The school was later moved to the site of the old Naval Observatory at 23rd and E. Streets, N.W., Washington, D.C. It survived until the Spanish-American War in 1898 dispersed both faculty and students. It was reopened in 1902 at the same location under the official title of "Naval Medical School."34 In addition to performing the functions of a postgraduate and orientation school for officers newly
appointed to the Medical Corps, it also took up medical research and will be mentioned again in that connection.The Naval Dental School was started in 1922, and like the Medical School, provided postgraduate instruction for dental officers and training for hospital corpsmen assigned to duty as dental technicians. The Dental School provided also a laboratory for the construction of special prosthetic appliances, and clinical service to the Naval Hospital, Washington, D.C. Lack fo funds caused it to be discontinued for some three years in the early 30's. It was reestablished in 1934, and transferred to the National Naval Medical Center in 1942.35
A Hospital Corps Officers School was commissioned at the National Naval Medical Center, Bethesda, Maryland, on July 12, 1943, and in 1945 was redesignated the United States Naval School of Hospital Administration. Its main purpose was to train Hospital Corps (later Medical Service Corps) officers in procurement, commissary, accounting, and other aspects of naval hospital administration.36
During the war, enlisted men selected for the Hospital Corps were given basic training for Medical Department duties at schools located near recruit training centers. Their training was continued on assignment to a medical activity. Nurse training was principally of the "on-duty" type in hospitals, although some were given additional schooling in psychiatry and dietetics, and instruction to qualify them as flight nurses.
The ever-increasing demand for physicians and dentists in the fleet and ashore during World War II made it impossible to send all newly commissioned officers to the Medical and Dental Schools. Instead they were ordinarily given a short indoctrination course at a naval hospital or other major medical activity before proceeding to their duty stations. A relatively small number were ordered back to the Naval Medical School for specialized instruction in such subjects as submarine or aviation medicine. Generally, those selected were career physicians in the regular Navy rather than Reserve officers. This situation also prevailed in the case of dental officers.
Naval hospitals had their beginning in an Act signed by President John Adams in 1798, creating a fund for the relief of sick and disabled merchant seamen by deducting twenty cents a month from their wages.37 The following year the Act was extended to the naval service and the Medical Department Facilities
Secretary of the Navy was directed to deduct the same amount from the pay of naval officers, seamen, and marines in the United States Navy.38 In 1811, by "an Act establishing Navy hospitals" the naval contributions were placed in a separate Naval Hospital Fund and to this fund were added all fines imposed on officers and men.39 The hospital fund retained its identity and was administered as a separate trust fund until June 15, 1943, when Congress, in an Act to simplify naval accounting procedures, abolished the fund and combined it with the general appropriation for the Medical Department.40Initially, the Secretaries of the Navy, Treasury, and War were constituted commissioners of "Navy Hospitals" and were authorized to procure hospital sites and erect buildings thereon. The Navy hospitals so provided were unsatisfactory temporary buildings. The first permanent hospital buildings were erected at Norfolk and received patients in 1830. Naval hospital and their equipment were thereafter kept fairly well in step with the Navy's needs and with advances in medical science, although lack of funds always left much to be desired in the plans of BuMed and of progressive officers of the Medical Corps Several new hospitals were built with National Recovery Administration funds during the early 30's. In December 1941, there were 18 continental naval hospitals in commission plus one each at Pearl Harbor and Canacao in the Philippines. Some very productive planning for expansion was, however, under way, which bore fruit shortly after the attack on Pearl Harbor.
Mention has been made of the postgraduate schools in medicine and dentistry operated by the Bureau which formed part of the training of Medical Department personnel. With a view to integrating postgraduate education with opportunities for practical experience, the Secretary of the Navy by General Order No. 70 of June 20, 1935, established the Naval Medical Center in Washington at 23rd and E Streets, N.W., to consist of the Naval Medical School and the Naval Hospital, although both had been located there for some years. The Naval Dental School was included in the Naval Medical Center the following year, although it also had been established as early as 1922. However, even before the declaration of the national emergency in 1939 it was recognized that space was lacking in that area to expand the outgrown facilities of the Center. After a number of recommendations by the Surgeon General the construction of a new Medical Center was authorized by Congress,41 at Bethesda, Maryland, a few miles outside of Washington. The new National Naval Medical
Center, consisting of a Naval Hospital, Naval Medical School, and Naval Dental School, was commissioned about three years later on February 5, 1942. The Bureau of Medicine and Surgery then moved from the Main Navy Building into the buildings vacated by the old Medical Center at 23rd and E Streets, N.W.A laboratory for medical research was not included in the original plans for the Medical Center at Bethesda, but largely through the persistent efforts of the Surgeon General, such a facility under the name of Medical Research Institute was added to the program and was ready for commissioning on October 27, 1942, about a year after the completion of the Naval Hospital itself. The place that it filled in the administration of BuMed and of the Navy Department during World War II will be covered under the subject of "Medical Research."
During the 1939-1941 preparedness period much was done to increase the facilities of existing naval hospitals. Plans were also made to take over hotels, private sanatariums, and schools, so as to gain time over the construction fo new hospitals. For example, a former hotel was commissioned the United States Naval Hospital, Corona, California, within ten days after the attack on Pearl Harbor.42 Before the end of the war, some 31 additional naval hospitals and 15 special or convalescent hospitals were established and 8 annex units were added to existing hospitals.
The procedure for establishing a new naval hospital consisted of a number of steps varying somewhat with individual cases. Normally, the Bureau looked to the District Medical Officer to keep it advised of the situation with respect to naval hospital needs in his district. This he did through the Commandant of the District. On receipt fo such a report the Bureau might direct its Inspector to confirm the reported need. Study and recommendation by the Planning Division of BuMed followed, leading finally to a decision by the Surgeon General. In connection with the study by the Planning Division, a board consisting of the District Medical Officer, a Bureau of Yards and Docks representative, and a BuMed representative usually also inspected the proposed location or locations. Finally the Surgeon General submitted all of the data with his recommendation to the Chief of Naval Operations.
If the latter approved, the papers went to the Federal Board of Hospitalization, the Coordinating Agency for Hospital Expansion Programs of the Armed Services. This board passed final judgement on the project giving due consideration to the suitability of the proposed hospital as a possible postwar facility for the Veterans Administration. After final approval
by the Secretary of the Navy acquisition of property and the placing of contracts for the construction of buildings could begin.The Construction B ranch of the Bureau of Yards and Docks, in cooperation with the Design Section in the Planning Division of BuMed, had usually done a considerable amount of work on the plans before the project had received the formal approval of the Secretary. Acquisition of real estate, completion of plans, and placing of contracts by the Bureau of Yards and Docks followed quickly. Until July 20, 1942, the legal aspects of real estate transactions were handled by the Judge Advocate General, but after that date the Bureau of Yards and Docks took over this work. The Bureau of Supplies and Accounts had the responsibility for the financial aspects of the projects.
Before World War II, the standard interval between centers of hospital beds was 8 feet. This was reduced to 6 feet when a shortage in beds became imminent, and increased the capacity of the hospitals considerably. In June 1939, the total patient census in naval hospitals was 4,124. By June 1941, this had risen to 7,723.43 On December 7, 1941, the continental naval hospitals were caring for 7,558 patients which left only the small margin of 879 beds available for war casualties.44 By 18945, the average patient census in naval hospitals reached 90,635.45
Mobile and Base Hospitals. In 1939, the need for some type of prefabricated, transportable, self-maintaining hospital was visualized and led to the design of what came to be known as U.S. naval Mobile Hospital No. 1. This was a 500-bed completely equipped general hospital under canvas, with self-contained power, water, commissary, laundry, and repair facilities. Procurement of the material and equipment for the project was handled by the Medical Supply Depot, Brooklyn. The hospital operating personnel were ordered to the Supply Depot for temporary duty and given a course of indoctrination while the hospital was being packaged preparatory to shipment to the Naval Station, Guantanamo, Cuba, where it was assembled and was ready to receive patients within 13 days after arrival of the shipment.46
Lessons learned from this experimental unit resulted in the substitution of pre-fabricated buildings for tents. It was found also that much time could be saved by loading last the items needed first in setting up the hospital, and by clear and informative labeling of created items. Inaccurate labeling often caused crates to he opened, when the contents were not
needed until much later. This experience proved valuable when mobile and base hospitals were provided for combat areas. The second mobile hospital set up at Aeia Heights on the island of Oahu was near enough to completion to receive many of the wounded from the Pearl Harbor attack. When hospitals were established at advanced bases and lost some of their mobile characteristics they were termed base hospitals.The capacity of hospitals of this kind ranged fro 200 to 2,500 beds. Some had as many as 300 buildings. The number of medical officers attached ranged from 40 to 54, dental officers from 1 to 4, Hospital Corps officers from 1 to 5, and Hospital Corpsmen from 235 to 500.47
Fleet Hospitals, as some mobile hospitals were designated after mid-1944, were generally larger than Base Hospitals, and were located in areas further to the rear of the combat zones. Fleet Hospitals were under the command of a medical officer whose immediate superior was the commander of the Fleet to which he was attached; whereas Base Hospitals were part of a commissioned Naval Base.48
The Fleet and Base Hospitals, particularly in the Pacific, proved their worth from the standpoint of providing temporary hospitals in the forward and rear areas. However, they never achieved the degree of mobility desired and needed by a rapidly moving front.49 To meet this objection, BuMed planned eight "Special Augmented Hospitals" as an intermediate between the field station and the Fleet and Base Hospitals. They were of 200 to 400 bed capacity and designed to bring services, such as X-Ray, surgery, laboratory, dentistry, etc. to the immediate combat vicinity. Cessation of hostilities prevented these special augmented hospitals from being given practical service tests. Five such units were landed at Okinawa, but only two actually received patients before Japan surrendered.
Naval Dispensaries may be defined as those medical facilities on shore other than naval hospitals provided for the immediate and usually temporary care of the sick and injured. During World War II, those treated in dispensaries consisted of naval personnel, dependents of naval personnel, and at navy yards and other shore establishments civilian employees of the government entitled to first aid treatment. At overseas dispensaries, particularly in North Africa and on the islands of the Pacific, treatment was also extended to natives. Dispensaries ranged in size from first aid stations manned by a single hospital corpsman to installations with as many as 500 beds.
Activities designated "U.S. Naval Dispensaries," for example, those in the Navy Department, Washington, D.C.; San Francisco, California; Miami, Florida; and a few others provided only out-patient treatment. Such dispensaries were under the direct management and technical control of BuMed, with a medical officer in command. Station and Base Dispensaries, while coming under the Bureau's technical control, were the management responsibility of the base or station commanding officer.The bulk of the patient load in continental naval dispensaries consisted of dependents. In May 1945, there were some 3,700,000 dependents of naval personnel. For that same month, 127 hospitals and 218 dispensaries reported 179,153 dependent's out-patient visits; 4,846 dependents admitted to naval hospitals; 2,609 admitted to civilian hospitals but attended by navy doctors.50
Medical Facilities Afloat. Hospital ships of sorts formed a part of large fleets from earliest times. Such ships accompanied the Spanish Armada to the English Channel in its ill-fated challenge of English sea power in 1588.51 Their purpose was, however, more to serve as isolation wards for contagious diseases in order to protect the fleet against epidemics than for routine care of the sick and injured.
American hospital ships, that is, floating general hospitals, date from the Civil War. They were first used by the Federal forces operating on the Mississippi River and its tributaries. A capture Confederate side-wheel steamer was commissioned as the United States Navy Hospital Red Rover in December 1862. The vessel was described in a report to Commodore Foote as "the most complete thing of the kind that floats, and is in every way a decided success. . . . She has bathrooms, laundry, elevator for the sick from the lower to the upper deck, amputating room, nine different water closets, gauze blinds to the windows to keep the cinders and smoke from annoying the sick, two separate kitchens for sick and well, a regular corps of nurses, and two water closets on every deck."52
The war with Spain in 1898 saw the Navy making more extensive use of hospital ships. This led to the controversy at the turn of the century, between the Medical Corps and the Line, over the question of command of hospital ships. Surgeon General Presley M. Rixey reasoned that since a hospital ship is in fact a hospital afloat, a medical officer would be best qualified to command such a ship; furthermore, that placing hospital
ships under the command of combatant officers might, under the Hague and Geneva Conventions, disqualify them for immunity from attack.53The Bureau of Navigation replied that medical doctors having neither training nor experience in navigation and ship handling were, therefore, not qualified for command.54 BuMed countered with a proposal to place navigation, deck, and engineering functions in the hands of a competent sailing master and a civilian crew, because the "command is eminently a non-combatant one."55
The Secretary of the Navy and the President endorsed Surgeon General Rixey's views, and the Chief of the Bureau of Navigation resigned in protest. In a letter to the Secretary, dated 4 January 1908, President Theodore Roosevelt wrote:
"The hospital ships of the Navy will hereafter, unless otherwise directed by Congress, be placed under the control and command of medical officers of the Navy, their navigation being exclusively controlled by a competent sailing master and civilian crew, the sailing master having the complete responsibility for everything connected with the navigation of the ship . . . Military surgeons, including naval surgeons, have special knowledge of hospital ships, and they have in addition certain military duties of command, organization drills and discipline, just as do officers of the line, awarding punishments and being guided and governed in these military duties by the same regulations that guide and govern officers of the line. The command of hospital ships should unquestionably be vested in a medical officer, and no line officer should be aboard it."56
The Secretary of the Navy received an affirmative reply from the Attorney General on the legality of medical officers commanding hospital ships, and Navy Regulations were changed accordingly.57
President Roosevelt's decision was altered by a Congressional Act of 29 August 1916 which allowed navigation, deck, and engineering duties in a hospital ship to be assigned to line officers of the Naval Reserve Force,58 but left the command with a medical officer.
The only naval hospital ship to cross the Atlantic to Europe in World War I was the USS Comfort. She sailed late in the war and fear of German submarine attack compelled her to travel under convoy as a transport without distinguishing marks. A line officer commanded the Comfort in passage, but upon arrival at Brest, France, command reverted to the medical officer.59
In 1920, the pendulum swung back to line officer command of hospital
ships by a decision of the Judge Advocate General in reviewing the findings of a court-martial. The case concerned a naval reserve line officer serving in a hospital ship who was court-martialed for disobeying a lawful order of his superior in that he refused to sign a noon position report when ordered to do so by the commanding officer, a medical doctor. The Judge Advocate General held that "medical officers cannot exercise command in the line or other staff corps either by law or existing regulations and therefore the accused was not guilty of having disobeyed the lawful order of his superior officer.60 As a result, Navy Regulations were again changed, and the controversy ended with only the line considered eligible for command of hospital ships.61 Post World War II regulations specify that the senior medical officer in a hospital ship is under command of the Commanding Officer. In the hospital spaces of the ship, the Commanding Officer normally limits exercise of command to security, discipline, watertight integrity, etc. He does not have control, within the hospital spaces, over such matters as medical technical procedures, administration, and organization, or accountability fo funds allotted to the medical department.62The Navy went into World War II with only two hospital ships in service, not enough to handle the requirements of even the war in the Pacific. Steps were immediately taken to use hulls under construction by the Maritime Commission for development into hospital ships. By the end of the war, there were twelve naval hospital ships in operation, most of them built in that way. Decisions as to the topside arrangement of the ships and as to their machinery installations were the responsibility of the Bureau of Ships. Details as to the arrangement and equipment of the Medical Department spaces were worked out jointly by the Contract Design Branch (Conversion Section) of BuShips and the Planning Division (Hospital and Ship Plans Section) of BuMed, with the former having the technical responsibility for the naval architectural and shipbuilding features.63 Copies of all plans and specifications covering Medical Department spaces were sent to BuMed for comment. BuMed assigned a medical officer to duty at the works of the shipbuilder as an inspector to ensure compliance with Medical Department requirements with respect to ventilation, elevators, operating room arrangements, lighting and all other features having a bearing on the suitability of the ships for hospital use.
Sick Bays. On combatant ships sick bay bed space was provided at the beginning of the war for two percent of the ship's complement. For troop transports this was later increased to three percent, but remained as before throughout the war for other ships, except fo assault ships (APA's). The latter had up to 75 or more beds and a staff of 16 medical officers, so as to be able to give immediate medical attention to the wounded during an offensive operation. Space assignment and arrangements for sick bays and were handled in a manner similar to that described for hospital ships. Procurement, except for strictly medical and dental equipment, was the responsibility of BuShips.Air-Conditioning. BuMed and BuShips had a strong common interest in the ventilation of ships and in temperature and humidity control of working and living spaces below decks. their interest lay not only in the comfort of personnel but also in providing working conditions that would not impair the efficiency of men who had to spend much of their time in confined spaces. BuShips' interest extended still further to the temperature control of magazines and to humidity control in spaces housing equipment requiring a dry atmosphere.
Air-conditioning was recognized as th solution to most of these problems, but even after this branch of engineering had reached the practical stage in shore installations it was not an immediate answer to the Navy's needs because equipment suitable for shore use was not sufficiently rugged to stand up under seagoing conditions. improvements were gradually made so that by the middle 30's air conditioning was successfully applied to submarines. Experimental installations were also made on the larger surface ships, beginning with spaces where human efficiency was a prime consideration. It was next extended to spaces where comfort of the occupants was of particular importance, such as in sick bays and on hospital ships. By the time the huge naval shipbuilding program of 1940 was under way many of the weaknesses of the early installations had been corrected through close cooperation between BuShips, BuMed and the manufacturers, with the result that air-conditioning could be applied extensively on new ships. Air-conditioning played a substantial role in mitigating one of the prime discomforts of life on naval ships. It promoted the morale of the operating forces, particularly of the submarine forces.
Some of the major responsibilities and characteristics of the Bureau of Medicine and Surgery and of the Medical Department of the Navy have been covered in the foregoing pages, particularly those that are unique to BuMed Organization
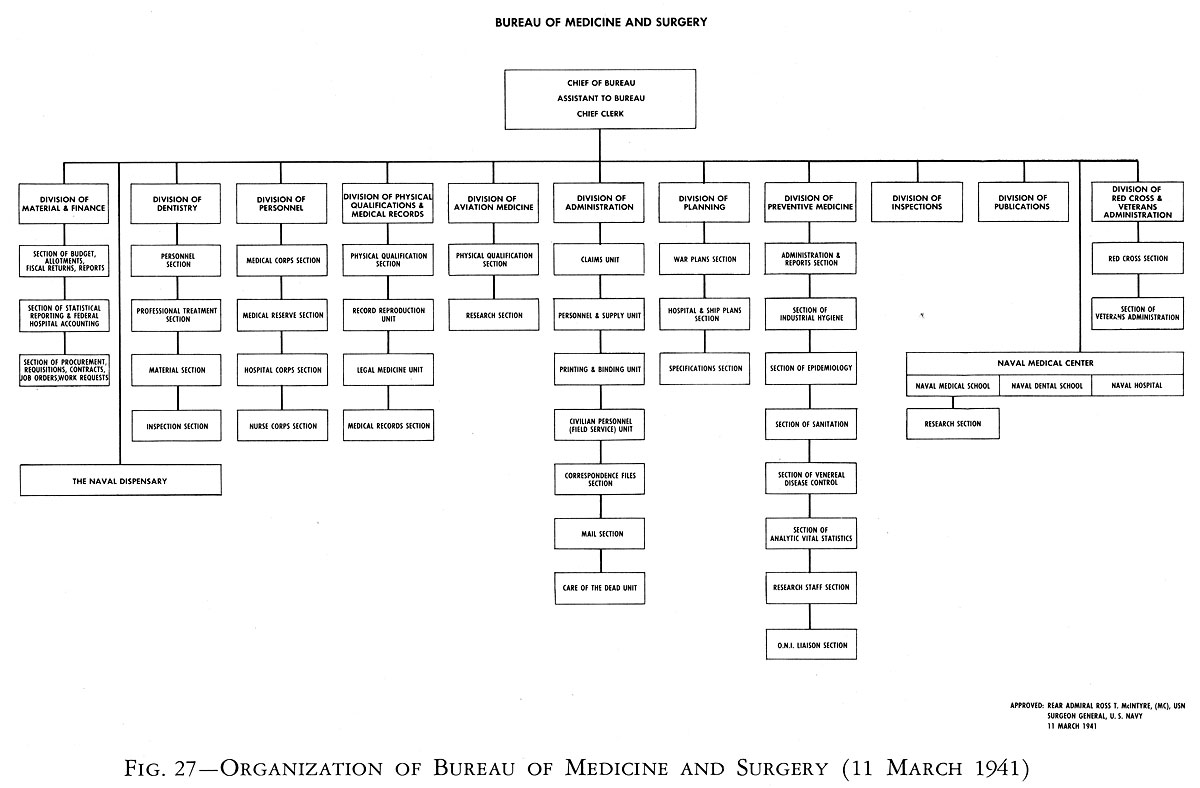
Fig. 27--Organization of Bureau of Medicine and Surgery (11 March 1941)
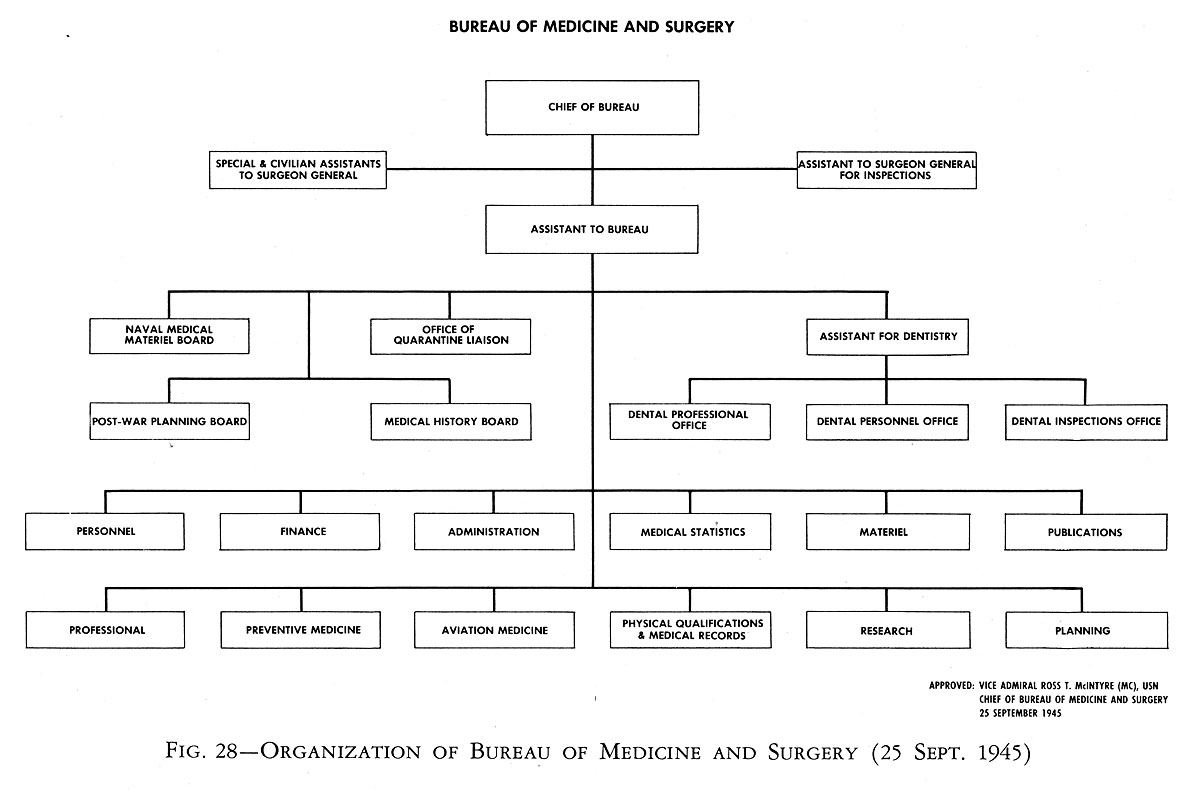
Fig. 28--Organization of Bureau of Medicine and Surgery (25 Sept. 1945)
the medical profession. There were, however, many steps in carrying out BuMed's broad mission of "caring for the sick and the injured" that differed little from the procedures that other branches of the Navy Department had to follow in carrying out their missions. In providing medical supplies for the Navy, BuMed had a task, for example, that in kind was much the same as that of the technical bureaus, even though BuMed's expenditures for such purposes were very small as compared to those of the Bureau of Aeronautics or the Bureau of Ships. To carry out its mission BuMed had to be soundly organized and had to observe the principles of efficient business management just as did the other bureaus and subdivisions of the Navy Department.The organization of the Bureau as of 11 March 1941 was as shown on Figure 27, with its functions distributed among eleven divisions. The heads of these divisions reported to the Chief of Bureau through the Assistant Chief, as did also the head of the Naval Dispensary of the Navy Department and the Commanding Officer of the National Naval Medical Center, Bethesda. The nature of the responsibilities of the respective divisions is indicated by their titles.
The organization as of September 25, 1945, that is, at the end of the war, is shown on Figure 28. This is the organization that may be said to have evolved out of the experience of World war II. It will be noted that it consisted of twelve major divisions, an Assistant for Dentistry, four boards, an Assistant for Inspections, and of the Chief's Special Civilian Assistant. The chart indicates that the heads of the twelve major divisions and the boards had access to the Chief of Bureau through the Assistant Chief. The Assistant for Inspections and the Special Civilian Assistant reported directly to the Chief of Bureau without going through the Assistant Chief. actually, it was the practice of the Surgeon General when in Washington to see, personally, the heads of the divisions every day, as will be described presently.
The firm of management engineers, previously mentioned, who had been employed by Secretary Knox to study the organization and administrative practices of the Navy Department, began making a survey of BuMed early in 1942 and submitted a report to the Chief of the Bureau under date of July 25, 1942, covering their findings and recommendations. This report contains the reasons for many of the changes that were made. A few observations on this report as a whole are in order as they will highlight the principal organizational and administrative problems that the Bureau had to meet.
The survey was thorough and covered all of the Bureau's activities. It contains the statement that the management engineers "received whole-hearted cooperation from all people contacted in the Bureau." The state
of readiness of the Bureau and of the Medical Department of the Navy to carry out its mission when Pearl Harbor was attacked on December 7, 1941, is summarized as follows:64"Faced with its mission of safeguarding the health of the Navy and Marine Corps, the Bureau began, in 1939, to prepare for the present world conflict. Into its expansion program went the foresight and untiring efforts of Medical Department personnel, with the result that when Pearl Harbor was attacked December 7, 1941, the Medical Department was ready for almost any eventuality. This state of readiness was accomplished through careful planning and through having an organization to execute the plans."
The survey invited attention to many problems well known to career naval personnel, some that are in fact inherent in all government-operated activities; the paucity, for example, of capable administrative type executives, especially among the civilian personnel; the existence of points of duplication and friction that make it difficult to effect improvements in organization and management in th Government services; deep-seated resistance and prejudices in some instances to obviously desirable changes in methods and procedures which often had their roots in the vested interests of the personnel concerned. There were mentioned also the more specific current handicaps to efficient operation such as poor working conditions due to overcrowded office spaces, shortage of modern office equipment, inadequate restaurant facilities and other factors adversely affecting morale. These were in part the result of the enormous increase in the Bureau's workload following the declaration of the national emergency.
In their surveys the management specialists always stressed the importance of distributing the work of all activities, no matter how large, among as few basic groups as possible, so as to keep to the minimum the number of individuals who had to have direct and frequent access to the Chief. This, in order to avoid burdening the Chief with unnecessary details, and to give those, who ha to seem him regularly, the opportunity for full statements on important matters without hurrying through their visits. Conserving the time of the Surgeon-General was of particular importance during World War II, because he served in the dual capacity of Chief of the Bureau and White House physician. Rear Admiral McIntire divided his time about equally between the two positions.
The management engineers recommended for the Bureau a maximum of five groups whose heads would have regular and direct access to the Chief. The functions of the respective groups were to be personnel, planning, research, accounting, and procurement of material. At the time of their report each of these functions was scattered among a number of
divisions. In the case of research, six divisions dealt with the subject in one form or another. Actually the carrying out of this recommendation seems never to have been completely achieved as the organization at the end of the war shown on Figure 28 still shows twelve main divisions. The situation was, however, much improved by redistributing, concentrating, and coordinating the functions of all the divisions. An outstandingly competent Assistant Chief of Bureau greatly mitigated the disadvantages of dealing with so many divisions.65Special Civilian Assistant. The management consultants also attached great importance to the assignment of a civilian assistant for the chief of the Bureau with experience in office management. In their report they recommended that this assistant be of the "energetic, engineering type"; that he need not belong to any branch of the medical profession. This individual's principal duties would be to evaluate the organizational structure of the Bureau, the adequacy of its facilities, the appropriateness of the distribution of its functions, the preparation of regulations for the guidance of the organization, the measures for coordinating the efforts of the various divisions, and the steps to be taken for getting qualified civilian personnel to fill the key supervisory positions in the organization.
They pointed out that merely initiating improvements in such matters would not be enough; that the arrangements made should envisage progressive and continuing need for improvement so as to keep the organization and its administrative procedures in step with changing conditions; that such work can never be considered finished. The Special Assistant was given administrative rank a step above the division heads with direct access to the Surgeon General. It was appreciated that an individual capable of making a success of the position would have to be a man of considerable ability, tact, patience, and firmness, but the position was finally filled satisfactorily under date of October 21, 1942.66
The former Administration Division was reorganized, making it the implement for putting into effect the studies and recommendations of the Special Assistant. Its routine responsibilities consisted of keeping the Bureau staffed with efficient civilian personnel, of providing mail, messenger, and correspondence filing service, and of looking after the innumerable housekeeping, maintenance and supply needs of the Bureau. The creation of the position of Special Assistant caused some overlapping with certain functions being performed by the Chief Clerk of the Bureau. On June 10, 1943 the tile of Chief Clerk was dropped as most of his duties had been
absorbed by the Special Assistant.67 An additional civilian assistant to the Surgeon General was appointed as his legal advisor who followed up legislative matters for the Bureau.In connection with the organizational changes being studied at that time a Finance Division was established, having the responsibility for the preparation of the Bureau's budget, of passing on requests for funds coming from the field, for exercising budgetary controls, prescribing accounting methods, auditing expenditure vouchers, and for maintaining property and fiscal records. These functions had theretofore been scattered among various divisions in the Bureau.
No change was made in the Publications Division which prepared, edited, and distributed Bureau literature, such as the Naval Medical Bulleting, special brochures and pamphlets, and served as the central point for the dissemination of Bureau information.
Professional Divisions
Some of the most important functions of BuMed were of a highly professional nature and did not lend themselves to incorporation in those segments of the organization dealing with the business management of the Bureau. In the pre-war organization these functions were scattered among various divisions. After considerable study they were segregated under a number of separate divisions. A Professional Division was established to maintain a continual study of the professional needs of the Medical Department of the Navy, and to make recommendations for the improvement of its practices. It maintained close liaison with the civilian medical profession and other Government medical agencies, so as to keep the Navy in step with medical advances in all fields.
A Division of Preventive Medicine was established and given cognizance over all matters involved in medical prophylactics. It made studies and recommendations on policies, medicines, and through to further the cause of disease prevention, especially with respect to diseases prevalent in the combat areas. It was also a function of this Division to maintain close liaison with other Government agencies, and with the Committee for Medical Research.
The medical needs of aviation had reached a stage of such importance that specialization in that field was indicated. A Division of Aviation Medicine was set up. This division maintained close liaison with the Bureau of Aeronautics and with aviation medicine in the Army. It supervised the development of psychological screening tests used in selecting
aviators. Better flying gear and clothing, and air-sea rescue equipment came under its cognizance. It helped write instructions for air evacuation of the wounded, high altitude training of aviators, and rehabilitation of war weary pilots.
Assistant for Dentistry. The segregation in Figure 28 of the adiminstration of BuMed's dental activities under an Assistant for Dentistry will be noted. The part that dentistry had come to play in carrying out the mission of the Medical Department of the Navy in maintaining the health of the Navy had grown in importance with the years. But the position of officers in the Dental Corps, organization and administratively, had not been resolved to the satisfaction of that Corps. On board ship, for example, dental officers had been striving for independence from the Medical Department and for co-equal status with the medical officer in authority and responsibility. Proposals had actually been made in the past for setting up dentistry as a function of the Navy Department independent of the Bureau of Medicine and Surgery.68 Most dental officers did not, however, go that far and believed that by giving full recognition to the education, training, and capabilities of naval dentists adjustments could be made in their status that would lead to greater contentment of dental officers with their position, responsibilities, and authority in the Navy.69
A number of changes were accordingly made in the organization of the Bureau to give dentists a feeling of greater responsibility and usefulness. Under date of May 25, 1945, and Assistant for Dentistry at a level above that of a Division Head was established. All functions having to do with the Dental Corps and dentistry were placed under this Assistant, and distributed among three divisions, the Dental Professional Office, the Dental Personnel office, and the Dental Inspection Office.
Further organizational changes were made early in 1946, after the passage of Public Law 284 (79th Congress) which directed the establishment of a Dental Division in the Bureau. The intent of the legislation was to concentrate the administrative responsibilities of the Naval Dental Service in one group on the same organizational level as other major groups in the Bureau and field activities.70
Assistant for Inspections. Before the war the inspection of medical facilities was the responsibility of two inspectors, one for the East Coast and one for the West Coast. During the war a third was added for the control parts of the United States. The Surgeon general felt, however, that inspections had become too routine and in a large measure perfunctory, and that this important function was in need of revitalizing. The question was given lengthy consideration because inspections, if carried out vigorously, were bound to encroach on the responsibilities of the District Medical Officer. The change was, however, placed in effect under date of August 24, 1945, when an Inspector General--an assistant to the Surgeon General--was appointed, who reported directly to him. It became the responsibility of the Inspector General, not only to make on-site inspections, but also to peruse carefully the reports of District Medical Officers and to bring to the attention of the Division Heads of the Bureau any matters under their cognizance needing attention.
A word is appropriate at this point on the method followed by the Surgeon General in administering the affairs of the Bureau. Rear Admiral McIntire considered his role to be that of policy maker and Bureau representatives at all conferences above bureau level or on Capitol Hill. He maintained personal contacts with the Secretary of the navy and other high level civilian executives, the chief of Naval Operations, other bureau chiefs, the Army Surgeon general, and normally appeared personally before Congressional committees, instead of being represented by subordinates. All of this meant that he had to keep in close touch with everything going on in the Bureau. To this end, when he was in Washington, he saw each of the Division Heads every day, to discuss problems, to make policy decisions and to keep up to date on BuMed programs. He desired action letters to be only one page long, with the important points in the first paragraph. Staff papers or studies were longer. He allotted two hours each week to the study of such papers, and two hours to technical research information coming from the National Research Council, the Committees of Medical Research and other sources.
The Deputy Surgeon General, Rear Admiral Luther Sheldon, was the executive and expediter for the Bureau. In this capacity ge checked frequently on Divisions Heads to see that agreed upon policies and programs were being carried out with all possible dispatch.
Medical Statistics
In September 1943 the Surgeon General appointed an Advisory Committee on Vital Statistics. Included in the Committee were five outstanding statisticians and public health specialists from civil life. The
Committee was to advise the Surgeon General on what changes to make in the Bureau's practices with regard to vital statistics in order to make them more useful.71 the Committee submitted a comprehensive report on January 17, 1944, expressing the opinion that the purpose of medical statistics should be (a) to provide quantitative knowledge of the incidence, nature, and distribution of illnesses, and other factors affecting the health of naval personnel; (b) to assemble such statistical data as necessary for the more efficient operation of medical facilities and services and for the assignment of medical and dental personnel on the basis of their qualifications; (c) to prepare such data as necessary for planning and forecasting naval medical needs under conditions of war and of peace; and (d) to provide for the systematic dissemination of such information to the various elements of the naval establishment in accordance with their requirements.72One of the important conclusion reached by the Committee was that the lack of a single point in the Bureau for receiving, analyzing, evaluating, coordinating, and distributing statistics militated greatly against their intelligent preparation and effective use. The Committee considered that the statistics were of such value as to justify setting up a division having exclusive cognizance of such matters and that the division should be headed by an individual of recognized ability and professional standing in this field. A Medical Statistics Division was finally set up under date of August 1, 1945.
Medical Supply
Supplying medicines to the Navy as an organized service began in a small way in 1850 when one room was assigned in the Naval hospital, Brooklyn, for packaging, storing, and distributing a few drugs and medical supplies to the Navy. In 1906 a separate building was erected on the Naval Hospital grounds for this purpose and was designated the United States Naval Medical Supply depot. It had laboratory equipment for testing medical supplies and served as the principal procurement, storage, and shipping center for medical supplies to ships and the naval shore establishments. The Supply Depot was expanded gradually and by 1940 had net storage space of about 120,000 sq. ft. It was making annually some 8,750 tests and inspections and filling some 4,960 requisitions representing about 2,835 tons of shipping weight. Within a hear additional buildings had to be erected. By the end of World War II the Medical Supply
Depot, Brooklyn, together with its Annex at Edgewater, New Jersey, had over one million sq. ft. of storage space.
At the beginning of the war the organization of the Bureau did not concentrate control of medical matériel in any one office. A Division of Material and Finance, a Division of Planning, and the Medical Supply Depot, Brooklyn, all had a hand in logistic planning, determination of requirements, and the procurement, inspection, and distribution of medical supplies. This resulted in conflicts of authority and duplication of effort. In the summer of 1943 the Surgeon General had his Special Assistant, jointly with the Management Engineer of the Navy Department, make a survey of the situation, with the result that on November 10, 1943 the Matériel Division was established as a unit of the Bureau in one of the buildings of the Supply Depot. An office in the Bureau in Washington provided liaison with the other divisions of the Bureau. The location of the Matériel Division in Brooklyn had the dual advantage of close proximity to the Medical Supply Depot and to the head offices in New York of the leading manufacturers of pharmaceuticals and hospital equipment. The Matériel Division took over from the Supply Depot its former functions of long range planning, stock control, and authority for making changes in the supply tables.
Naval Medical Material Board
A Naval Medical Material Board had been set up in December 1942, consisting of eminent authorities in civil life to advise the Surgeon General on such matters as the adoption of new drugs, medicines, and the latest advances in medical and dental equipment and techniques.73 This Board kept in close touch with the research activities of the Bureau, and received assistance from the National Research Council.
For many years the Bureau of Medicine and Surgery had followed the practice of publishing a stock catalogue known as the medical supply tables listing those items of medical and dental supplies carried in stock at the Medical Supply Depot and available for issue to the naval service on requisition. Only drugs and medical supplies in accepted use by the civilian medical and dental professions were stocked. The tables were, however, under continuous scrutiny and revision in order to keep naval medicine and techniques up to date. Normally naval hospitals, dispensaries, and the medical departments of ships were not permitted to experiment with new drugs and equipment not listed in the supply tables, but special
purchases could be made on specific authority of the Bureau or in conformity with regulated procedures. In this way BuMed avoided ultra-conservatism in the use of new drugs and techniques, and at the same time kept the Medical Department of the Navy from precipitate action in taking up new drugs without some background of experience. Excessive stocks were also avoided in this way. During the war this policy underwent considerable modification, especially with respect to drugs and medicines needed to combat diseases endemic to certain areas.
BuMed made very effort to support the naval forces with adequate medical supplies, but there were times when there was a shortage of some items. The Bureau then sent notices to overseas area commands, listing the actual and prospective shortages, with estimated dates when stocks were expected to be ample again. The Bureau controlled the issue of essential articles of this kind, giving priority to the areas most in need of such items.
The Medical Supply Depot, Brooklyn, continued to be the central point for the procurement, testing, packaging, and distribution of medical supplies. It had branch depots at Mare Island, California; Charleston, South Carolina; San Diego, California; with a number of satellite stations and storehouses. The Depot had the responsibility also for procuring, assembling, and maintaining a stock of hospital corps ouches, battle dressings cases, first aid kits, and the medical equipment for boat boxes. The Matériel Division exercised technical and management control over all of these activities and the naval medical storehouses in the continental United States. In effect, it took over the function of procurement that had theretofore been largely handled by the Medical Supply Depot, Brooklyn. Medical supply procurement rose from a money volume of $1,000,000 for the fiscal year 1940 to a volume of about $120,000,000 for the fiscal year 1944.
Arrangements for vastly increased medical supply production and expansion of manufacturing facilities constituted a very important phase of the material program. As in other areas of the war effort, adequate supplies depended on availability of strategic and critical materials.
The Surgeon General designated an experienced chief pharmacist a his personal representative and liaison with the War Production Board. The liaison officer's duty was to handle all matters concerning priority materials and material allocations in connections with the production of medical supplies and equipment. By the foregoing arrangement with WPB, BuMed was able to secure an adequate share of strategic and critical materials and productive capacity to meet medical requirements.
The Bureau made numerous direct contacts with manufacturers to compel them to live up to contract specifications and to induce them to
improve equipment to meet Navy needs. It may be mentioned that joint pressure from BuShips and BuMed resulted in the development by private manufacturers of the first mobile laundry.
The problem of BuMed in making medical supplies actually available to the fighting forces at the front was common to all Bureaus with their supplies. There were often ample stocks in continental storehouses and in the pipelines, but no way of getting them to the places where needed. A step toward solving the problem for medical supplies was taken by the Service Force, Pacific during September 1942 when small stocks of the most important items were placed on tankers for distribution to ships in the forward areas. This innovation worked so well, although in quantity it was inadequate to meet the situation, that space was increased on AK's (Auxiliary Cargo Ships) for medical supplies of all kinds. When new Ak's were built, special consideration was given to storage space for medical supplies. The result was that by the end of the war the stock of such supplies in overseas storehouses could be reduced from a basis of meeting the requirements of 100,000 men for 30 days to 60,000 men for 30 days.
A number of barges under the control of the Service Forces were also fitted out to store and issue medical supplies. The largest of these floating storehouses stocked over 1500 items, in quantity sufficient to care for 150,000 men for 30 days. The barges were stationed near fleet anchorages or at advanced bases and were moved forward with the fighting front, thus avoiding the tie-up in the rear areas of medical supplies urgently needed at the front.
Shipment of Blood
Making whole blood available for transfusion at the fighting front in the Pacific was one of the outstanding logistic achievements of BuMed during the war. The Surgeon General was a member of the Central Committee of the American National Red Cross before Pearl Harbor. In 1940 the Bureau began discussing with Red Cross officials the procurement and use of whole blood for military purposes, and with the National Research Council methods for procuring, preserving, packaging and shipping whole blood to the fighting fronts. These studies were carried on in collaboration with the Surgeon General of the Army.
To the Red Cross was assigned the responsibility for procuring blood from the general public; to the Army dealings with manufacturers for processing whole blood into plasma; and to the Navy the processing of serum albumin. During the early years only plasma could be shipped long distances, as it was impossible to ship whole blood and to have it arrive in war theatres suitable for transfusions. Late in 1943, however, a preservative known as the ACD solution was developed, which kept whole blood in useable condition for a limited time.
The first shipment of whole blood left the west coast by air for Guam on November 16, 1944. Guam became the center for the Navy's distribution of whole blood to all forces in the Pacific. Arrangements had to be made for re-icing at Pearl Harbor and Kwajalein, and for discarding at Guam containers showing excessive destruction of red blood cells or evidence of contamination. In preparation for an amphibious operation hospital ships were provided with blood for distribution to the participating forces. An LST was specially equipped for storing blood and for making ice for packing it. Specially equipped trucks transported the blood to the front. The Marines used blood from a mobile bank in the Iwo Jima and Okinawa operations.
Planning Division
Some mention has already been made of the emergency planning undertaken at the outbreak of the war. A study in the summer of 1943 by the Special Assistant and the Management Engineer of the Navy Department, of the handling of BuMed supply functions led to the reorganization of the Planning Division, and to clarification of its duties and responsibilities. Greater stress was placed on coordinating medical support plans with basic war plans. In collaboration with other bureaus it made studies of Medical Department facilities ashore and on ships. It worked closely with CNO and Headquarters of the Marine Corps to determine Medical Department requirements in amphibious operations. A Postwar Planning Board was also established under date of November 13, 194374 to develop programs for the intelligent disposition of excess Medical Department property, facilities, equipment, and supplies which were certain to remain on hand at the end of the war.
Medical Research
Much space has justifiably been devoted in all histories of World War II, whether dealing with operations or administration, to the influence of contemporaneous scientific research and development on the conduct and outcome of the war. A chapter will be found in this work on "Research and Development," in which the story of the mobilization of civilian scientists and the part they played in weapon development and medical research is told in some detail. It is, nevertheless, appropriate even at the risk of some repetition to outline briefly in this place some aspects of medical research, as the administration of this activity was one of the important tasks of the Bureau of Medicine and Surgery during World War II. The object of medical research was to devise practicable means of
protecting the health of personnel against the innumerable environmental and occupational hazards to which they were exposed in the Armed Forces. The motivation in this endeavor was humanitarian as well as the conservation of the manpower of the nation.
The Medical Department of the Navy had, for many years, made notable, even though not extensive, contributions to research in naval medicine in such fields as tropical medicine, deep sea diving, aviation medicine, the habitability of ships, and other fields involving living at sea. Research in these areas was, however, carried on largely by individual medical officers who had become interested in the subjects and so far as lay within their power, had devoted their careers to the study and development of these specialties. The Naval Medical School for the postgraduate instruction of naval medical officers, had had cognizance of medical research since the establishment of the school. Research was conducted under the overall direction of the Bureau although no one division in the Bureau had exclusive responsibility for research. There were, in fact, no well organized facilities and procedures for carrying on such investigations until the creation of the Medical research Institute as part of the Naval Medical Center at Bethesda in 1942. The Research Institute was placed in commission on October 27, 1942, some 8 or 9 months after the naval hospital and other facilities at the Center had gone into service, as it was not included in the original plans for the Medical Center. The inclusion of a medical research laboratory was timely, as it came at a period when the mobilization of civilian scientists began to play an important role in the war effort.
When World War II broke out in Europe in September 1939, a group of the leading scientists in the United States began urging the mobilization of civilian scientists to assist the armed services in preparing for national defense, as it seemed likely that the United States would eventually be drawn into the war. Under the leadership of the President75 of the National Academy of Sciences, these men presented their views to the Council of National Defense and to President Roosevelt. As a result the National Defense Research Committee (NDRC) was set up on June 27, 1940, under the National Defense Council, with the approval of the President. After devoting a year to organization and to exploring the best approach to the many problems that would be encountered in developing the full potentiality of such a mobilization, Executive order No. 8807 of June 28, 1941 was issued by the President, establishing the Office of Scientific Research and Development (OSRD) within the Office for Emergency Management of the Executive Office of the President and
placing under it as its working body the NDRC to deal with weapons and other instrumentalities of war.
During the year that elapsed after the formation of the NDRC the feeling grew that something similar to research on weapons should be undertaken also in the field of military medicine. A Committee of Medical Research (CMR) paralleling the NDRC was accordingly set up by the Executive Order establishing the OSRD. The NDRC and the CMR became the working machinery of the OSRD76 for mobilizing the civilian scientists for the purpose of giving authoritative advice to the armed services on the potentialities of science in solving many of their problems, and for filling the gaps in existing knowledge needed to exploit to the fullest the destructiveness of weapons on the one hand and the conservation of the health of the fighting forces on the other. So far as the Navy Department was concerned the CMR dealt almost exclusively with the Bureau of Medicine and Surgery, whereas the NDRC worked with all bureaus, including BuMed. The CMR consisted of seven members, one of whom was appointed by the Secretary of the Navy as the representative of the Navy Department.77
Details of the operating procedures of the OSRD and of its two working committees will be found in the chapter on "Research and Development," but it is appropriate at this point to describe briefly how the medical research interests of BuMed were correlated with CMR. After the creation of that committee, BuMed took stock of its own organization in this field and concentrated all of its research activities in a single division; formerly these activities were scattered among several divisions and in the Naval Medical School. The single division provided a focal point for liaison with CMR. The head of the division was also appointed the Navy Member of the CMR.
The Committee for Medical Research conducted all of its programs on a team basis. An example will best illustrate the method that was followed. Malaria was, during the early months of the war in the Pacific, one of the most serious hazards to the health of the fighting forces. Stocks of quinine were dwindling rapidly, with no satisfactory substitute in sight. The CMR took up the development of anti-malarials as one of its earliest projects by setting up the "Board for the Coordination of Malarial Studies." Drugs and control measures for the many-sided attack
on malaria were developed through the team effort of clinicians, chemists, parasitologists, pharmacologists, toxicologists, immunologists, and manufacturing laboratories. Some 15,000 compounds were synthesized and their actions studied in the search for effective anti-malarials.78
Similar methods were used for handling other projects. The team members were in some cases individuals, but more often laboratories, and special research groups. This method not only made it easier to get the best minds to work on any given problem, but also got results in the shortest possible time. The successful outcome of the many projects undertaken in this way testified to the wisdom of the policy followed by the CMR and supported by BuMed. World War II was the first major war in history in which casualties due to enemy action exceeded those due to disease; this, in spite of the fact that in World War II the combat areas included many regions saturated with factors of high morbidity.
As soon as the Medical Research Institute opened its doors in October 1942, it began to participate as a team member n many CMR programs. In some projects the Bureau and its laboratory, the Institute, took the leading role as the Navy was often in an advantageous position to undertake certain types of research because it had facilities and other resources not available to civilians. For example, the large aggregation of personnel, under military control at training stations, afforded excellent opportunities for studies in communicable diseases.
The Institute concentrated on the development or evaluation of devices and practices for use by the fleet. The invention, development, and evaluation of measures for the survival of shipwrecked personnel were among its most important research activities. Extensive studies and improvements were also made in such things as protective clothing, body armor, desalination of sea water, aviation oxygen equipment, measures for insect control, vaccines, night vision, treatment of tropical diseases, etc. Shortly after the war the Institute participated in the Bikini atomic bomb tests, and has since then contributed greatly to studies on the biological effect of radiation.
Panels of outstanding medical doctors and scientists in the medical fields were appointed to act as consultants to the Surgeon General on the many special medical problems that arose during the war. The civillians on these boards gave their services to the government without compensation other than the usual travel and per diem allowances for their out-of-pocket expenses.
Summary
In World War II the performance of the Bureau of Medicine and Surgery in carrying out its mission was outstanding by any standard of
measurement. The Surgeon General, Vice Adm. Ross T. McIntire, MC, USN, in his Foreword to the History of the Medical Department of the U.S. Navy in World War II gave a few statistics, showing the progress made in modern times in caring for the sick and wounded. He said that in early wars 50 percent and more of all wounded men died as the result of their injuries. In World War I, out of every 100 wounded 90 recovered; in World War II, out of every 100 wounded 98 recovered. Recovery in World War II from certain types of injuries was even more striking. For example, deaths from wounds of the head, chest, and abdomen were about 65 percent lower than in World War I.
Basically the great improvements in saving the lives of wounded men was due to the enormous advances made in medicine and allied sciences just before and during the war. Among these were the development of new drugs, vaccines, serums, and hospital equipment, advances in surgery; the therapy of treating shock and exhaustion by the transfusion of blood, and the prevention and control of epidemic diseases in combat areas. But medical progress alone would not have been enough to ring about these remarkable achievements. It required also the presence at the front of trained men and women dedicated to the care of the sick and wounded. Procurement of the wonder drugs, the blood plasma, the hospital equipments depended finally on the efficient administration by the Bureau of Medicine and Surgery of the Medical Department of the Navy.
The magnitude alone of the expansion in personnel that was involved in the effort was one of the administrative difficulties that the Bureau had to meet. In June 1940 there were 92 civilians and 48 military personnel on duty in the Bureau. At the height of the war in the early summer of 1945 these numbers had risen to 633 civilians and 670 military personnel. The entire Medical Department of the Navy at the beginning of the war consisted of less than 14000 persons. In 1945, when the Navy had reached its greatest expansion, it consisted of 179,225 people.
Table of Contents
Previous Chapter (11) * Next Chapter (13)
Footnotes
1.U.S. Stats. at Large, 1st-5th Congresses. 1 Stat. 721-723. "An Act to Regulate the Medical Establishment," March 2, 1799.
2. U.S. Stats. at Large, 18th to 23rd Congress, 4 Stat. 313, "An Act for the Better Organization of the Medical Department of the Navy of the United States." May 24, 1828.
3. An illustration of the range of BuMed activities is the White House physician. In recent years he has often been detailed from medical officers of the Navy. In February 1935, Captain Ross T. McIntire, (M.C.), USN, later Vice Admiral, was so designated, and remained President Franklin D. Roosevelt's physician until the latter's death in 1945. McIntire was appointed Chief of the Bureau of Medicine and Surgery on December 1, 1938, and served as such until his retirement on April 1, 1946. Duty of a similar nature was that performed by Captain George W. Calver, (M.C.), USN, later Rear Admiral, who was detailed as the physician to Congress and served in that capacity throughout World War II. Both the White House physician and the physician to Congress provided very useful liaison relationships between the Navy Department and the legislative and executive branches of the Government.
4. Louis H. Roddis, A Short History of Nautical Medicine (New York, Paul A. Hoeber, Inc., 1941), pp. 214-215.
5. U.S. Stats. at Large, 55th Congress, 30 Stat. 1006. A SecNav General Order of August 31, 1846 had previously established relative rank on a slightly different basis than the 1865 Regulations referenced above.
6. W.J.C. Agnew and N.L. Saunders, "The Navy's Medical Department," War Medicine, Vol. I, (May 1941), p. 12.
7. U.S. Stats. at Large, August 22, 1912, 37 Stat. 344.
8. SecNav Report, 1945, p. A-85.
9. Statistics of Navy Medicine (Sept. 1945), Vol. I, No. 1, p. 4.
10. Agnew, op. cit., pp. 13-14.
11. Agnew, op. cit., pp. 17.
12. U.S. Stats. at Large, 39 Stat. 572.
13. SecNav report, 1945, p. A-85.
14. U.S. Status. at Large, 61 Stat. 736.
15. Laws Relating to the Navy, Annotated, p. 4069.
16. Ibid., p. 4070. By an act of April 16, 1947, 61 Stat. 47, Title II, the Nurse Corps was made a regular Staff Corps of the Navy, with actual rank and Commissioned status.
17. SecNav Reports, 1917, 1918, 1919.
18. Rear Admiral P.S. Rossiter, (M.C.), USN, who preceded Rear Admiral McIntire as Chief of the Bureau, was very active in building up the Medical Corps Reserve.
19. Based on a statement made by Vice Admiral Ross T. McIntire, (M.C.), USN (Ret.), November 1, 1956.
20. Ltr from Director, Office of Defense, Health and Welfare Services to the President, with President's approval thereto, 30 Oct. 1941, BuMed QR/OM, 1942 (BuMed Files, National Archives).
21. BuMed QR/OM(122-40), 14 Jan 1942 (National Archives files).
22. Conversation with Vice Admiral Ross T. McIntire (MC), USN (Ret.), Sep 1955.
23. BuMed ltr Nav-1t612 EMJ in BuMed File QR/OM 1942, 15 Jan 1942; BuMed file QR/OM(9104), 31 Oct 1942 (BuMed Files, National Archives).
24. Exec Officer, P&A to Surgeon General, BuMed file QR/OM 1942, 11 Jan 1942 (BuMed Files, National Archives).
25. Procurement Directive 5-42, 28 July 1942, in BuPers Admin History, Vol. III, Part 2, Appendix, Vol. I.
26. BuMed P-14-2(023) G-MHF, 18 Feb 1943, (BuMed Files, National Archives).
27. BuMed QR/OM(122-40), S:CRM, 17 June 1943, (BuMed Files, National Archives).
28. BuPers Admin History, Vol. 4, Part 4, p. 161.
30. Statistics of Naval Medicine, Vol. 1, No. 2 (Oct. 1945), p. 5.
31. New York Herald Tribune, 8 Mar 1945.
32. Navy Department Press and Radio Release, 16 Apr 145 in Washington Post, 17 Apr 1945.
33. BuMed Admin. History, Vol. II, Part 2, p. 574.
35. BuMed Admin. History, Vol. II, pp. 583-590.
37. This Act was also the beginning of the U.S. Marine Hospital services renamed the U.S. Public Health Service in 1902.
38. U.S. Stats. at Large, 1 Stat. 729, Chapter 36, 2 March 1799.
39. Ibid., 2 Stat. 650, p. 26, 26 Feb. 1811.
40. Ibid., 57 Stat. 125, 15 June 1943.
41. Public Law 493 approved by the President April 26, 1939.
42. Legal difficulties in clearing the title prevented the Corona hospital from receiving patients until February 24, 1942, BuMed Admin. History, Vol. II, p. 283.
43. BuMed Admin. History, Vol. II, p. 106.
44. Ibid., Vol. II, pp. 266-267.
45. History of the Medical Department, World War II, I.
46. History of the Medical Department, World War II, Vol. I, p. 137. Mobile Hospital No. 1 was moved to Bermuda in September 1940.
47. A mobile hospital played an important role in China in giving support to Chinese guerillas mobilized under Captain Milton E. Miles, USN, with Captain Gordon B. Tayloe, (M.C.), USN, in charge of the hospital. The mobile hospital was moved from place to place, as necessary, to escape the Japanese forces.
48. BuMed Admin. History, Vol. II, p. 836.
49. Ibid., Vol. II, pp. 859-860.
50. Statistics of Navy Medicine (Sept. 1945), Vol. I, No. 1, p. 35. The term "dependent" means the lawful spouse, unmarried children under 21 years of age, and the mother and father of a member of the Navy or Marine Corps if dependent on such member.
51. "The Origin and Early Development of Naval Medicine" by W.L. Mann, U.S. Naval Institute Proceedings, Vol. 55, Part 2 (Sept 1929), p. 781.
52. Records of the Union and Confederate Navies, Sec. 1 Vol. 23, p. 153.
53. Report of Joint Board of Medical Officers and Endorsements Thereto, 24 Sept 1906," (BuMed Files, National Archives).
54. Ibid., 4th Endorsement, 4 June 1906.
55. Ibid., 6th Endorsement, 24 Sept 1906.
56. Roosevelt to SecNav, 4 Jan 1908 (BuMed Files, National Archives).
57. Attorney General to SecNav, 24 Aug 1909 (BuMed Files, National Archives), Surgeon C.F. Stokes was named commanding officer of the hospital ship Relief.
58. U.S. Stats. at Large, Chapter 417, 39 Stat. 589, Aug. 29, 1916.
59. BuMed ltr confirming dispatch orders of 9 Oct 1918 (BuMed Files, National Archives).
60. JAG review of case of Lieutenant Commander Athol H. George, USNRF, 6 June 1921 (BuMed Files, National Archives).
61. Change No. 2 to Navy Regulations, 1920 promulgated 1 November 1921.
62. United States Navy Regulations, 1948, Art. 1327.
63. BuShips memo to CNO(Op-29), EN10(112) Ser 110-1458, dated 13 May 1955. In this reference the following statement is made: "The informal liaison maintained between BuShips and BuMed appears to have worked well. This office knows of no objections having been raised against this system and knows of no adverse effects. The records available to this office indicate that all differences were resolved at bureau level."
64. "Survey of Administration, Bureau of Medicine and Surgery, Navy Department," by Booz, Fry, Allen & Hamilton, July 25, 1942, Chap. III, p. 64.
65. Rear Admiral Luther Sheldon, Jr. (MC), USN, was the Assistant Chief of the Bureau from June 26, 1940 to November 24, 1944.
66. Mr. A.F. Emch formerly Executive Secretary of the American Hospital Association, was commissioned a lieutenant commander in the Naval Reserve, and took over this position on October 21, 1942. After the war it was filled by a civilian.
67. Memo for Chiefs of Bureau Divisions from Rear Admiral McIntire, June 10, 1943, A3-4/EN(073-40). (BuMed Files, National Archives).
68. BuMed Admin. History, Vol. II, p. 88.
69.Chief, Dental Division to Chief BuMed, "Comment on Proposed Plan," April 1943, A3-4/EN 1942-June 1943 (BuMed Files, National Archives).
70. Subsequent postwar organizational changes established the office of General Inspector, Dental Activities directly under the Chief of the Bureau on the same level as the General Inspector, Medical Activities. The Dental Division was placed under an Assistant Chief of Bureau for Dentistry. A Planning and Analysis Branch, a Professional Branch, a Personnel Branch, and a Reserve Branch made up the Dental Division. In accordance with the organizational responsibilities throughout the Bureau the heads of these Branches were given the same relative responsibilities as the Directors of other divisions. The organization of ships and stations was also changed to establish dental departments under a dental officer who reported directly to the Commanding Officer. The dental officer reported to the medical officer only for battle stations, but in 1948 even that exception was removed.
71. Memo Chief BuMed to Heads of Divisions, BuMed E-AIJ, A304/EN (073-40) of Sept 23, 1943.
72. "Evaluation of the Vital Statistics Function of the Bureau of Medicine and Surgery," Advisory Committee 1944, Naval History Division Files.
73. BuMed Admin. History, Vol. II, pp. 99-100.
74. Acting Chief of Bureau memo to Chiefs of Divisions, BuMed-E-AIJ, A3-4/EN(073-40) 13 November 1943 (BuMed Files, National Archives).
75. Frank B. Jewett, the Head also of the Bell Telephone Laboratories.
76. Dr. Vannevar Bush became the Director of the OSRD; Dr. James B. Conant, President of Harvard University, the Chairman of the NDRC; and Dr. A Newton Richards of the University of Pennsylvania, the Chairman of the CMR.
77. Rear Admiral Harold W. Smith, MC, USN, served as the Navy Department Representative on the CMR throughout the war. He was also the head of the Research Division of the Bureau of Medicine and Surgery.
78. History of the Medical Department of the U.S. Navy in World War II, Vol. I, p. 316